1 / 5
| Model NO. | W03 |
| Condition | New |
| Usage | Fracture Fixation |
| Using Site | Waist, Tibial, Radius, Femoral, Humeral |
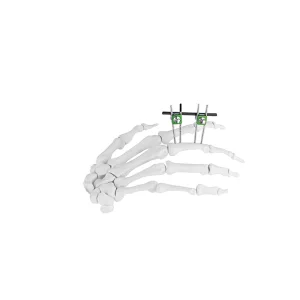
| Type | External Fixator |
| Application | Orthopedic |
| Group | Adult |
| Material | Aluminum |
| Transport Package | Sterilized, PE Bag, Carton Package |
| Specification | Customizable |
| HS Code | 9021100090 |
| Production Capacity | 1000pieces/Week |

Physicians have been using external fixation to treat fractures for more than 2000 years after being first described by Hippocrates as a way to immobilize the fracture while preserving soft tissue integrity. The fixator design and biomechanics have changed dramatically over the years, but the principles remain the same. The primary goal of external fixation is to maintain the length, alignment, and rotation of the fracture. External fixation can serve as provisional fixation or definitive fixation purposes.
Both methods can be performed in conjunction with partial internal fixation if necessary. It is important for orthopedic surgeons at a trauma center to be familiar with the techniques and principles of external fixation for various fractures of the upper extremity, lower extremity, and pelvis.
Fracture healing physiology largely depends on the mode of fixation and level of stability. With absolute fracture stability such as compression plating, the bone will undergo primary intramembranous bone healing. On the other hand, relative fracture stability, such as external fixation, results in secondary enchondral bone healing. There are also several ways to alter the external fixation construct to make the fracture more or less stable.